Introduction

Retinopathy of Prematurity (ROP) occurs due to abnormal growth of blood vessels in an infant’s eye. During development, blood vessels grow from the central part of the retina outwards. This process is completed few weeks before the normal time of delivery. However in premature babies, it is incomplete. If blood vessels grow normally, ROP does not occur. On the contrary, if the vessels grow and branch abnormally the baby develops ROP.
The incidence of ROP in India is between 38-51.9% and it is as high as 80 – 100% in infants weighing <900 gms at birth or with a gestational age of <25 weeks. With the improved NICU care the incidence has increased.
Screening
Whom?
Birth weight <1750gm
OR
Gestational Age at <34 weeks
OR
Any premature baby with severe illness in perinatal period (RDS, sepsis, blood transfusion, IVH, apnoiec episodes, etc) need a retinal examination.
When?
Follow the 30 day strategy (i.e. the retinal examination should be completed at or before day-30 of life). Should preferably be done earlier (at 2 – 3 weeks of birth) in very low weight babies (<1200gm) or in babies with very low gestational age (<28 weeks).
How?
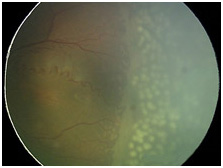
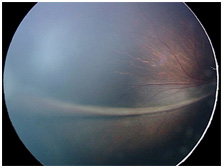
An ophthalmologist (Retina Specialist) can detect ROP by dilated fundus examination.
Indirect ophthalmoscopy is done to scan the entire retina and gauge the state of retinal maturity.
Management
The treatment in the form of lasers, intravitreal anti-VEGF injections or surgery is planned to reduce the Chances of unfavorable disease outcomes. Mild forms of ROP may resolve on their own without any active intervention. Severe forms of the disease on the other hand may need medical treatment as long as it is limited to stage 3. Surgical intervention is necessary once the disease reaches stage 4 or 5.
Follow up
Once treated, lifelong follow up (yearly) is mandatory. All other premature infants irrespective of having ROP yearly follow up till the age of 5 years is advisable.